After a tooth extraction, the surrounding bone naturally undergoes resorption if no intervention is performed. This physiological process can lead to a significant loss of volume, particularly on the buccal aspect, potentially compromising future implant placement and aesthetic outcomes. Socket management helps preserve the alveolar ridge, maintaining the necessary bone structure for predictable and successful rehabilitation.
Socket management should always be linked to the specific defect morphology, as the number of remaining socket walls and the integrity of the buccal bone significantly influence healing outcomes. Contained defects generally allow for simpler approaches with minimal intervention. Compromised sockets require more advanced techniques, including the use of membranes and grafting material. Adapting the treatment strategy to the defect type ensures optimal graft stability, supports predictable bone regeneration, and improves both functional and aesthetic results.
Extraction sockets are commonly classified based on the integrity of the surrounding bone walls, particularly the buccal plate. A frequently used classification distinguishes between intact sockets (Type 1), sockets with compromised buccal bone (Type 2), and sockets with severe defects or missing walls (Type 3). This classification is essential because it directly guides the treatment approach, ranging from simple socket preservation in intact cases to more advanced regenerative procedures in compromised defects. Understanding the socket type helps clinicians choose the most appropriate technique and biomaterials for predictable outcomes.
The choice of approach depends on defect morphology, treatment goals, and the desired level of intervention. In simple cases, a minimally invasive solution using collacone® may be sufficient to stabilize the clot. When long-term volume preservation is required, using cerabone® + HyA provides excellent stability.
For more complex defects, different concepts can be applied: a collagen-based approach with collprotect®, a non-resorbable d-PTFE barrier using permamem®, or a magnesium-based solution with NOVAMag® SHIELD for added structural support. Botiss portfolio allows clinicians to select the most appropriate and efficient solution for each socket type.
NOVAMag® SHIELD offers several key advantages due to its unique combination of rigidity and resorbability. As a metallic shield, it provides structural stability that helps maintain the regenerative space and preserve the buccal contour, supporting predictable bone formation. Its rigidity also makes it easier to position, particularly when tunneling between the periosteum and the remaining bone.
In addition, it promotes angiogenesis, contributing to a favorable healing environment. The technique is minimally invasive, as it does not require flap elevation or fixation, simplifying the surgical procedure. Finally, because the material is resorbable, there is no need for a second surgery for removal, improving patient comfort and overall treatment efficiency.
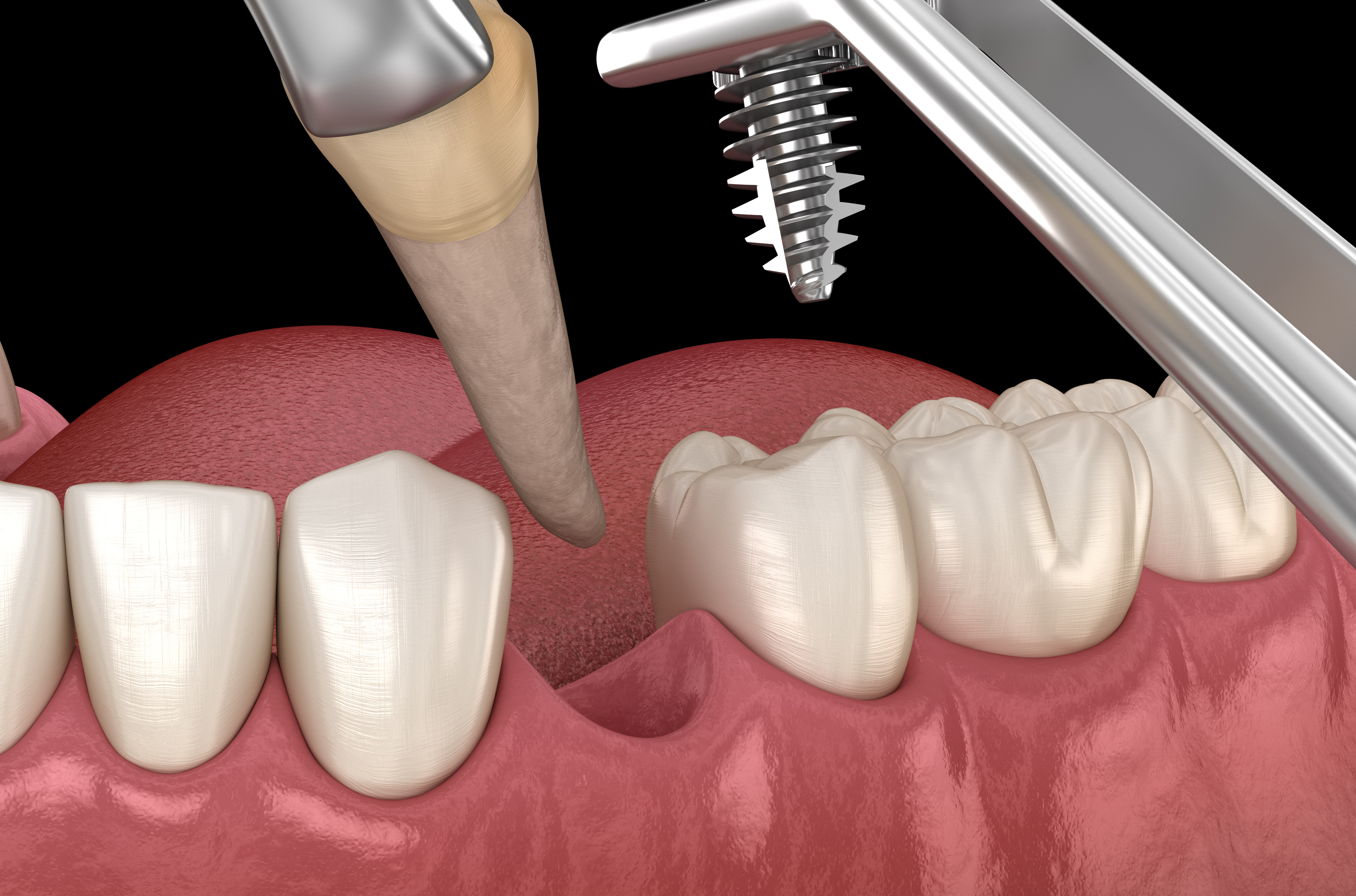
Yes, immediate implant placement is possible in selected cases with sufficient primary stability and absence of infection. However, in compromised sockets or when stability cannot be achieved, a staged approach with prior socket preservation is traditionally recommended.
Innovative solutions such as the NOVAMag® SHIELD are opening new possibilities, enabling immediate implant placement even in challenging or compromised sockets by providing additional stability and supporting hard tissue regeneration.
%20(1).jpg?width=1886&height=521&name=Header_Mobile_Socket-Management%20(1)%20(1).jpg "Header_Mobile_Socket-Management (1) (1)")